Psycholinguistic Screening for Cognitive Decline in Cancer Survivors: A Feasibility Study
Objectives: To test the feasibility of using psycholinguistic speech analysis as a proxy for cognitive function in men undergoing treatment for prostate cancer.
Sample & Setting: Audio-recorded speech samples were collected from 13 men enrolled in a parent study at the University of Kansas Cancer Center in Kansas City.
Methods & Variables: Audio-recorded speech samples, collected from clinical interviews and in response to a prompt question during the parent study at two time points, were evaluated to determine feasibility relationships between neurocognitive and psycholinguistic measures.
Results: Correlations between neurocognitive and psycholinguistic measures were identified for prompted speech, but the strength of relationships varied between time points. No relationships were identified in clinical interview speech samples.
Implications for Nursing: Feasibility was demonstrated for recording, transcribing, and analyzing speech from clinical interviews, and results suggest relationships between neurocognitive and psycholinguistic measures in prompted speech. If validated, psycholinguistic assessments may be used to assess cognitive function in cancer survivors. Advances in natural language processing may provide opportunities for automated speech analyses for cancer treatment–related cognitive decline.
Jump to a section
Prostate cancer primarily occurs in older men, with a mean age of 66 years at diagnosis; therefore, age-related comorbidities are common (Nguyen et al., 2015). Androgen-deprivation therapy (ADT) is used to treat prostate cancer throughout the disease trajectory by reducing testosterone to castration levels. Results related to the cognitive trajectory of men receiving ADT for prostate cancer remain mixed (Ryan et al., 2020). Estimates of treatment-related cognitive decline range from 47% to 69%, and cognitive decline may significantly affect functioning, ability to live independently, and quality of life (Gonzalez et al., 2015; Mundell et al., 2017; Nelson et al., 2008). With new interventions demonstrating the potential for overcoming negative cognitive and other effects of ADT, early identification of treatment effects on cognition is increasingly important (Manson et al., 2019). No standard of care exists for the assessment of cognitive changes in cancer survivors. Existing methods include the use of self-report measures, which may trigger follow-up assessments that involve a complex battery of abstract neurocognitive tests. This testing is conducted by trained psychometricians over two or more hours and may increase anxiety about cognitive abilities in older adults (Williams et al., 2014).
Because language production depends on intact function in a number of cognitive domains, spoken language reflects cognition that can be ascertained in everyday speech by measuring the complexity of grammar and vocabulary, as well as idea density in spoken language (Chen et al., 2009; Fernàndez & Cairns, 2010). Psycholinguistics and neurolinguistics—scientific disciplines that involve studying the psychological and neurobiologic factors linking cognition with language production and the effects of neurologic disorders on language—provide strategies designed to evaluate cognition as reflected in language (Fernàndez & Cairns, 2010) and act as the conceptual basis for this study. Specific patterns of language in everyday conversations can differentiate conditions ranging from normal aging and mild cognitive impairment (Aramaki et al., 2016) to Alzheimer disease (Kemper et al., 2001), vascular dementia (Williams et al., 2003), and other neurodegenerative disorders. Previous studies have suggested that changes in speech may be one of the earliest signs of cognitive decline, offering insight about cognitive deficits years before mild cognitive impairment (Eyigoz et al., 2020) or dementia (Beltrami et al., 2018). Advances in natural language processing show potential for automated analysis of spoken language, which may be used to assess cognition (Voleti et al., 2019).
Analysis of grammatical complexity and idea density of everyday conversations, as well as narrative responses to a prompt, have been used to characterize cognitive function and identify changes, which are confirmed with neurocognitive testing (Kemper et al., 2001). However, psycholinguistic measures have not yet been studied in the cancer survivor population. The goal of the current study was to evaluate the feasibility of using psycholinguistic analyses to measure language complexity in men receiving ADT and to examine relationships between language complexity and traditional neurocognitive measures. A secondary aim was to compare the use of psycholinguistic analysis between samples collected during clinical interviews and those collected through prompted elicitation questions.
Methods
The parent study, Staying Strong and Healthy for Androgen Deprivation Therapy for Men (NR014518, principal investigator: Maliski), is a randomized controlled trial of an intervention to minimize cardiovascular and metabolic risks of ADT through education, activity, and nutrition (Manson et al., 2019). The data collection was expanded for the current study to add self-report and objective measures to determine potential effects of ADT on neurocognitive function.
Recruitment
This study was approved by the institutional review board at the University of Kansas Medical Center in Kansas City. Thirteen participants were recruited from the parent study. Inclusion criteria were as follows: men aged older than 21 years, diagnosed with prostate cancer, starting or had started ADT for prostate cancer within the last three months, reinitiated ADT after being off treatment for longer than their previous ADT dosage, able to speak and read English, reachable by telephone, and able to travel to the university for data collection.
Procedures
During a six-month interval from July 2018 to November 2019, two speech samples were audio recorded during two regularly scheduled parent study visits. One five-minute recording was captured at each visit (time 1 and time 2) during the clinical interview for the parent study. In addition, answers to an elicitation (prompt) question that was designed to require thoughtful reflection were recorded. The elicitation question was taken from established protocols and was randomly selected from the following: “What person—living or dead, famous or not—do you admire the most and why?” and “What is the most significant event you’ve experienced? It could be about the best thing that ever happened to you or the worst thing that ever happened.”
Measures collected in the parent study included a battery of validated neurocognitive tests designed to measure the domains most likely affected by prostate cancer and cancer therapy. A summary of the psycholinguistic and neurocognitive measures used in the study is provided in Table 1. 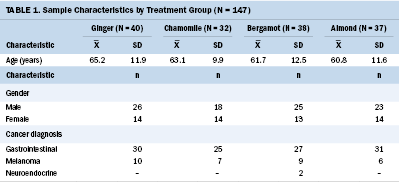
Four research assistants were trained in transcription using archived practice audio recordings until a minimum of 90% agreement was achieved for five practice recordings for each psycholinguistic metric. Recordings were transcribed verbatim and segmented into utterances (sentences or sentence fragments) using standards for psycholinguistic analysis (Kemper et al., 2001). Each utterance was coded for the number and type of noun–verb clauses it contained. A simple sentence includes one main noun–verb clause (e.g., “John [noun] called [verb] Mary”). Adding left- and right-branching clauses reflects greater complexity of the cognitive processes used to compose speech (e.g., “Before he went away [left-branching noun–verb clause], John called [main noun–verb clause] Mary to let her know the plan [right-branching noun–verb clause]”). Left-branching clauses are more cognitively demanding because the idea conveyed in the left-branching clause must be held in working memory while the remaining main clause is interpreted.
Coding was tabulated using Systematic Analysis of Language Transcripts software, version 2012. Two measures of sentence length were also computed: (a) mean length of utterance and (b) mean number of main clauses per utterance, left-branching clauses per utterance, and right-branching clauses per utterance.
Statistical Analyses
Because of the small sample size for this feasibility study (N = 13), nonparametric tests (Wilcoxon signed rank tests and Spearman’s correlation coefficients) were conducted and reported at each time point, with significance set at p = 0.05. The results should be interpreted with caution because of the small sample size and potential violation of assumptions for statistical tests.
Results
This feasibility study included data from 13 men ranging in age from 44 to 79 years, with a mean age of 66 years. Participants primarily were White (n = 12), in a relationship with a spouse or significant other (n = 12), and college educated (n = 10).
The correlations that were found between the neurocognitive and psycholinguistic measures are reported in Table 2. Only significant correlations in the elicitation (prompt) question sample were identified, and these varied between time 1 and time 2. No significant relationships between self-report measures of cognition and psycholinguistic measures were demonstrated. 
Results from the audio recordings that were collected as part of the parent study’s clinical interviews and responses to the elicitation (prompt) question were compared using Wilcoxon signed rank tests. Clinical interviews and prompted speech samples differed for the mean length of clauses per utterance (W = 62, p = 0.04), the number of left-branching clauses per utterance (W = 60.5, p = 0.03), and complete utterances (W = 26.5, p = 0.02). However, no significant correlations between neurocognitive and psycholinguistic measures were demonstrated in the study’s clinical interview speech samples.
Discussion
This study established feasibility for collecting language samples from men receiving ADT during routine cancer research study visits to evaluate cognitive changes occurring from treatment. Transcription and psycholinguistic coding were successful, reaching reliability of 90% or greater agreement for utterance segmentation and coding of clauses by graduate research assistants. Although a number of significant correlations were identified, the authors acknowledge that the results from this small feasibility study need to be validated in future research with larger and more diverse samples.
Significant correlations were also identified between the neurocognitive and psycholinguistic measures in the prompted speech samples, although these varied somewhat between time points. No relationships between semantic and grammatical complexity with self-reported measures of cognition were identified. This may be because of the small sample of participants (N = 13) who were assessed at each time point.
At time 1, verbal memory was correlated with grammatical complexity measures, including mean clauses per utterance (rs = 0.63, p = 0.02), and left- and right-branching clauses per utterance (rs < 0.78, p < 0.01 and rs = 0.61, p = 0.03, respectively). Verbal fluency also correlated with left-branching clauses per utterance (rs = 0.72, p = 0.01). The results indicated that increasing grammatical complexity, reflected in more complex utterances, mirrored higher scores for memory functions as assessed in the neurocognitive tests. Results on the timed Color Trails Test Part B were negatively correlated with the mean number of clauses per utterance and right-branching clauses per utterance (rs < –0.62, p < 0.03 and rs = –0.56, p = 0.03, respectively). The Color Trail Making Test Part B is a measure of executive function and processing speed, with higher scores indicating increased time needed to complete the test tasks. Higher language complexity correlated with poorer performance in executive function and processing speed domains in the current sample (Dugbartey et al., 2000).
At time 2, the Weschler Adult Intelligence IV Block Design—a measure of visuospatial ability—correlated with all of the psycholinguistic measures, including mean length of utterances in words, mean clauses per utterance, and main-, left-, and right-branching clauses per utterance (Strauss et al., 2006). These positive correlations of scores on neurocognitive and psycholinguistic measures were all in the anticipated direction (i.e., higher performance on neurocognitive tests correlates with more complex language utterances). The reason correlations were found for different psycholinguistic and neurocognitive measures at two time points is not clear and should be explored further.
A number of psycholinguistic and neurocognitive measures were significantly correlated in the elicitation (prompt) question data only. The lack of correlation with the clinical interview speech samples suggests that these two types of speech vary and that prompted speech provides greater sensitivity to cognitive function. Prompted speech requires the participant to think about and compose a response in an answer to an open-ended question. Therefore, prompted speech narratives rely more on cognitive and language processes (Kemper et al., 1989). In comparison, the responses to questions in research study interviews are likely brief and frequently include “yes” and “no” responses to specific, more finite questions. Because brief responses in research study interviews are less dependent on cognitive processes, they may be less reflective of cognitive processes.
This feasibility study provided preliminary results for psycholinguistic analysis of conversation to measure cognition in men receiving treatment with ADT for prostate cancer. If validated as a reliable and sensitive measure in cancer survivors, psycholinguistic analyses of speech samples could be compared over time to detect changes because of treatment effects, signaling a need for neurocognitive evaluation and potential interventions. If psycholinguistic analysis proves sensitive for identifying changes in cognition, an application may be developed at a low cost and made readily available across care settings.
Implications for Nursing
No standard of care is currently accepted to assess cognitive changes in cancer survivors, and issues exist for self-report measures and neurocognitive testing. Awareness of available assessment and screening tools and those under investigation is critical to nurses caring for cancer survivors. If relationships can be established between neurocognitive and psycholinguistic measures, psycholinguistic analyses may be used to assess cognitive function. Although the process of recording, transcribing, and coding speech samples is laborious and not feasible at the point of care, advances in automated transcription and natural language processing may provide potential tools for cognitive assessment in the future (Beltrami et al., 2018). A speech analysis application on a cell phone or other mobile device could be readily scalable in rural and other underserved areas where access to advanced neurocognitive testing is limited, which could improve care and potentially be used in telehealth visits. Using speech analyses to measure cognition, which is grounded in theories of psycholinguistics and neurolinguistics (Fernàndez & Cairns, 2010), has potential to fill a gap to improve care by providing a new tool for assessment of cognitive function. Identification of cognitive decline is the first step in initiating evidence-based interventions to prevent or minimize cognitive effects of cancer therapies and to initiate decision-making about therapy. 
Conclusion
If the relationships between neurocognitive and psycholinguistic measures in prompted speech suggested in this feasibility study are validated in ongoing research, psycholinguistic analyses may be applied to assess cognitive function and screen for cognitive changes. By assessing cognitive function in patients receiving treatment and cancer survivors, the need for time-consuming and stressful neurocognitive testing could be avoided.
About the Author(s)
Kristine Williams, RN, PhD, APRN-BC, FGSA, FAAN, is the E. Jean Hill Professor, Jamie S. Myers, PhD, RN, AOCNS®, is a research associate professor, Jinxiang Hu, PhD, is an assistant professor, Alana Manson, PhD, is a postdoctoral fellow, and Sally L. Maliski, PhD, RN, FAAN, is the dean of the School of Nursing and the Frank and Beverly Gaines Tipton Endowed Professor in Oncology, all in the School of Nursing at the University of Kansas Medical Center in Kansas City. This research was supported by the University of Kansas Medical Center (KUMC) Research Institute and the University of Kansas (KU) School of Nursing. The content is solely the responsibility of the authors and does not necessarily represent the official views of the KUMC Research Institute or KU School of Nursing. Williams, Myers, Manson, and Maliski contributed to the conceptualization, design, and manuscript preparation. Mason completed the data collection. Williams, Myers, Hu, and Maliski provided the analysis. Williams can be reached at kwilliams1@kumc.edu, with copy to ONFEditor@ons.org. (Submitted November 2020. Accepted March 10, 2021.)