Assessment of Cognitive Impairment and Complaints in Individuals With Colorectal Cancer
Purpose/Objectives: To assess cognitive function in individuals with colorectal cancer (CRC) and identify factors associated with cognitive effects.
Design: Cross-sectional, comparative design.
Setting: Midwest hospital.
Sample: Men and women with (n = 50) and without (n = 50) CRC.
Methods: Comparative and regression analyses were performed to assess the relationship between cognition and CRC.
Main Research Variables: Attention, cognitive control, and memory function were assessed with neuropsychological tests and self-report.
Findings: Compared to healthy volunteers, individuals with CRC performed worse and reported more problems on tasks requiring attention and cognitive control (p < 0.05). After controlling for covariates, poorer performance on tasks of attention and cognitive control was associated (p < 0.001) with having CRC, older age, and less education. In contrast, poorer perceived attention and cognitive control were associated (p < 0.001) with greater fatigue but not CRC.
Conclusions: Individuals with CRC are vulnerable to cognitive problems. In addition, older age, less education, and fatigue can increase risk for worse cognitive performance and self-reported cognition.
Implications for Nursing: Cognitive problems can profoundly affect an individual’s ability to function in everyday life and cope with cancer. Nurses should assess for cognitive problems in patients with CRC and intervene to reduce distress.
Jump to a section
More than 1.1 million individuals in the United States have a history of colorectal cancer (CRC) (American Cancer Society [ACS], 2014). Since the mid-1970s, advances in treatment and early detection have increased five-year survival rates by 14% for colon cancer and 20% for rectal cancer (ACS, 2014). Because of the prevalence of the disease and improved survival rates, understanding the effects of CRC and its treatment is critical to improving the quality of survivorship. A growing body of research suggests that individuals with non–central nervous system cancers can experience cognitive changes across the trajectory from pretreatment to as many as 20 years post-treatment (Koppelmans et al., 2012; Wefel, Vardy, Ahles, & Schagen, 2011). Potential mechanisms underlying cognitive changes include attentional or mental fatigue, psychological and symptom distress, inflammation, central neurotoxicity from chemotherapy, and changes in hormones (Merriman, Von Ah, Miaskowski, & Aouizerat, 2013). Individuals with CRC may be particularly vulnerable to cognitive changes secondary to increased proinflammatory activity associated with host–tumor interactions and cancer treatments, as well as central neurotoxicity from standard chemotherapy regimens containing fluorouracil (Adrucil®) (Cardinale et al., 2011; Han et al., 2008; Klampfer, 2011; Schaue et al., 2015; Tonini et al., 2002).
Cognitive abilities that appear to be most vulnerable to the effects of CRC and its treatments include attention, cognitive control needed for higher level executive function, and memory (Wefel et al., 2011). Attention is defined as the ability to selectively focus on information in the environment that is salient to a task while inhibiting other distracting stimuli (James, 1890; Kaplan & Kaplan, 1989; Petersen & Posner, 2012). Attention allows for efficient processing of immediate information from the internal and external environments (sensory, motor, and memory). Cognitive control shares a close functional connection with attention and is defined as the ability to actively maintain and process salient information in accordance with internal goals and inhibit distractions (Mackie, Van Dam, & Fan, 2013; Miller, 2000; Posner & Snyder, 1975). Cognitive control allows for engagement in extended goal-directed behaviors (Miller, 2000). Memory, specifically declarative long-term memory, is the ability to consciously access or recall stored information about specific personal episodes and facts about the world (e.g., objects, language) (Gazzaniga, Ivry, & Mangun, 2014; Squire, 2004). This form of long-term memory can support goal-directed behaviors by providing information or knowledge needed for carrying out an activity or behavior (Squire, 2004). Together, attention, cognitive control, and memory are necessary for executive functions including planning and carrying out activities, making decisions, learning, and effectively functioning socially (Gazzaniga et al., 2014). As such, even subtle alterations in these cognitive abilities can have significant consequences on an individual’s ability to make treatment decisions, cope with the uncertainty of cancer control, and adjust to multiple life changes.
Three research reports have examined cognitive changes in individuals with CRC (Andreis et al., 2013; Cruzado et al., 2014; Walker et al., 1996). Walker et al. (1996) used a computerized test of neuropsychological (NP) function to examine cognition in 17 individuals with CRC receiving treatment for advanced disease and found a significant decline in tasks requiring attention. Study findings were limited by a small sample size, attrition, lack of control groups, and self-report measures. Andreis et al. (2013) examined cognition in 57 individuals with CRC undergoing standard adjuvant chemotherapy (FOLFOX4) using a battery of NP tests and found no deterioration in performance from pretreatment to six months post-chemotherapy. However, the failure to find improvement from practice effects on some NP tests may suggest a subtle decline in function. Study findings were limited by lack of control group, cognitive self-report measures, and lack of statistical control of key covariates. Finally, Cruzado et al. (2014) examined cognitive performance in 81 individuals with CRC undergoing FOLFOX4 using a battery of NP tests and found cognitive deficits prior to therapy as well as a decline in cognitive performance from pretreatment to six months post-treatment. Cognitive domains affected included attention, cognitive control, and verbal long-term memory. Study findings were limited by attrition, no control group, and no cognitive self-report measures. Together, findings from these research reports suggest that individuals with CRC may be vulnerable to cognitive deficits, but the findings are difficult to interpret because of varying designs and NP assessments, small sample sizes, and limited analytic methods.
The review of the literature indicated that additional research was needed to investigate cognitive changes in individuals with CRC. Therefore, the purpose of the current study was to assess cognitive function in individuals with CRC and identify factors associated with cognitive effects. The study included (a) NP and self-report measures tailored to assess attention, cognitive control, and memory; (b) a healthy comparison group; (c) an adequate sample size; and (d) employed rigorous analytic methods to control for patient characteristics associated with cognitive decline.
Methods
Participants and Setting
An a priori power analysis indicated that 50 men and women with CRC and 50 men and women without CRC were needed to have 80% power to detect a medium to large effect size using an alpha of 0.05 for t test and multiple regression analyses (eight independent variables) (Cohen, 1992). The effect size is congruent with a previous study in individuals with cancer using similar cognitive measures (Jung & Cimprich, 2014). Participants were recruited from the University of Michigan Health System in Ann Arbor. Participants were assessed at one time point (a) within six months of a new diagnosis of primary or recurrent CRC (stage I–IV) or (b) within 12 months of a negative screening colonoscopy in healthy controls.
Eligible participants were aged at least 30 years, were literate in English, and scored 27 or more on the Mini-Mental State Exam, indicating no cognitive disorders (Folstein, Folstein, & Fanjiang, 2000). Participants were excluded for prior conditions that could influence cognition, including untreated or unstable psychiatric disorder, head injury, substance abuse, learning disability, and central nervous system disease. In addition, participants in the CRC group were excluded for a cancer diagnosis other than colorectal or skin cancer, and participants in the healthy comparison group were excluded for a cancer diagnosis other than skin cancer. From February 2011 to September 2012, 553 individuals with CRC were screened; 83 met eligibility criteria and 50 consented to the study and completed the cognitive assessment. Healthy controls were recruited consecutively from a colonoscopy screening clinic during the same period of time.
Measures
A battery of domain-specific NP tests and self-report measures was used to limit the time of testing and patient burden. Theoretical perspectives of attention and memory guided the selection of measures.
The Attention Network Test (ANT) is a theoretically derived measure of attention with supporting behavioral and neuroimaging studies and divergent validity (MacLeod et al., 2010; Wang et al., 2005). In this computerized NP test of attention, participants are asked to determine if an arrow in the center of the screen points to the left or right (Fan, McCandliss, Sommer, Raz, & Posner, 2002). The central arrow is accompanied by flanking arrows or neutral marks (straight line with no arrow head) that point in the same direction, point in the opposite direction, or are neutral. In addition, the central arrow is accompanied by alerting and spatial cues that provide information on when or where the arrows will occur, respectively. Attention is assessed by measuring accuracy and response times, and how responses are influenced by flankers, alerting cues, and spatial cues. Test-retest reliability scores on executive or cognitive control network scores range from 0.77–0.81 (MacLeod et al., 2010). The ANT is a sensitive instrument in patients with cancer (Jung & Cimprich, 2014).
The digit span (DS) test is an NP test of attention and cognitive control that asks participants to repeat a random series of numbers in a given order (DS forward [DSF]) or in a reverse order (DS backward [DSB]) (Lezak, Howieson, Bigler, & Tranel, 2012). The score is the number of digits repeated correctly before two failed attempts in each condition. Test-retest reliability scores range from 0.66–0.89 (Lezak et al., 2012). DS is a sensitive instrument in individuals with cancer (Jung & Cimprich, 2014; Small et al., 2011).
The Trail Making Test (TMT) is an NP test of attention and cognitive control that asks participants to draw a line to connect consecutively numbered circles (TMA) or consecutively lettered and numbered circles alternating between the two (TMB) (Reitan, 1979). Scores include the time in seconds taken to complete each task and a difference score. Test-retest reliability scores range from 0.74–0.85 (Giovagnoli et al., 1996). TMT is a sensitive measure in individuals with cancer (Wefel et al., 2011).
The Rey Auditory Verbal Learning Test (RAVLT) is an NP test of verbal memory that asks participants to recall words from a 15-item word list (list A) for five trials, followed by a second 15-item list of words (list B), and then immediate and 30-minute delayed recall of list A (Lezak et al., 2012). Because the word lists exceed typical estimates of short-term memory span, recall trials of the RAVLT are considered to be tests of long-term, verbal memory. Scores include the 30-minute delayed recall. Test-retest reliability scores for the delayed recall trial of the RAVLT range from 0.51–0.81 (Lezak et al., 2012). Word list measures such as the RAVLT have been found to be a sensitive measure in individuals with cancer (Wefel et al., 2011).
The Attentional Function Index (AFI) is a self-report questionnaire consisting of 13 items on which respondents rate their effectiveness of their function on common tasks requiring attention and cognitive control from 0 (not at all) to 10 (extremely well) (Cimprich, Visovatti, & Ronis, 2011). Scores are the average of all 13 items. The AFI has an internal consistency coefficient ranging from 0.76–0.94 (Cimprich et al., 2011). In the current study’s sample, the internal consistency coefficient for the AFI was 0.91.
The Everyday Memory Questionnaire (EMQ) is a self-report questionnaire consisting of 28 items on which respondents rate their frequency of memory lapses for a specific activity from 1 (not at all in the past month) to 7 (several times a day) (Cornish, 2000). Scores are the sum of the 28 items. The EMQ has an internal coefficient of 0.9–0.91 in adults (Cornish, 2000; Royle & Lincoln, 2008). In the current study’s sample, the internal consistency coefficient for the EMQ was 0.9.
The Profile of Mood States–Brief Form (POMS-BF) is a self-rating scale consisting of 30 words that describe feelings (e.g., tense). Respondents are asked to read the list of words and rate how they have been feeling in the past week on a scale of 0 (e.g., not at all tense) to 4 (e.g., extremely tense) (McNair, Lorr, & Droppleman, 1992). The anxiety, depression, and fatigue subscales have internal consistency coefficients from 0.78–0.94 in individuals with cancer (Cimprich, 1999; Cimprich & Ronis, 2001; Lehto & Cimprich, 1999). The anxiety, depression, and fatigue subscales were used in the current study’s analysis, and the internal consistency coefficients were 0.76, 0.88, and 0.81, respectively.
Procedures
The Institutional Review Board of the University of Michigan Medical School approved the current study. The principal investigator (PI) obtained informed consent from all study participants. Following consent, NP testing and self-report questionnaires were administered and scored by the PI. Testing was done in a private area, and procedures were as follows: (a) RAVLT immediate recall trials; (b) ANT, DS, and TMT objective measures in random order; (c) RAVLT delayed recall trial; (d) AFI, EMQ, and POMS-BF self-report measures in random order; and (e) demographic questionnaire. Time to complete testing was 60 minutes.
Data Analysis
Data were analyzed using SPSS®, version 22.0. Chi-square tests for independence and independent-samples t tests were used to describe the sample and to determine the adequacy of matching individuals with and without CRC on possible covariates and group differences in cognitive variables. Regression analyses were used to assess the relationship between CRC diagnosis and cognitive measures, controlling for key covariates. A composite score of attention and cognitive control, referred to as the attention composite score, was computed for some analyses by standardizing raw scores on DS and TMT using the sample mean and standard deviation of the measures, reversing scores on the TMT so that higher scores on both measures reflected better performance and summing the z scores. Composite scores of subtests for cognitive domains may improve the reliability of findings and have been used to describe cognitive impairment in individuals with cancer (Bender et al., 2013; Cimprich & Ronis, 2001; Jansen, Dodd, Miaskowski, Dowling, & Kramer, 2008; Lezak et al., 2012; Von Ah et al., 2012).
Results
Sample Characteristics
Sample characteristics are presented in Table 1. Participants ranged in age from 36–79 years, with a mean age of 56 years. Groups did not differ on gender, age, education, race, presence of chronic health problems, employment, or income status. For female participants, the groups did not differ on menopausal status or hormone replacement. However, the groups differed on psychoactive medications, with more individuals in the CRC group compared to the healthy group taking such medications (p = 0.00). Psychoactive medications included analgesics, antidepressants, muscle relaxants, and sedatives.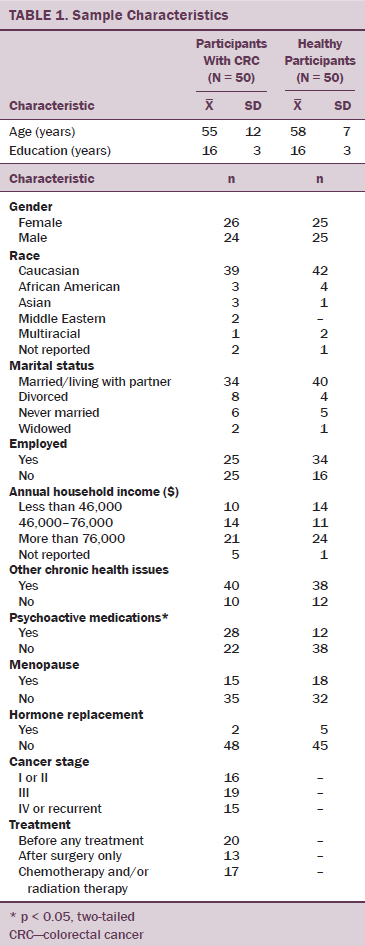
Individuals with CRC were assessed within six months of a diagnosis of new or recurrent CRC. All participants were diagnosed with invasive adenocarcinoma and were proportionately distributed across localized and more advanced stages of disease (American Joint Committee on Cancer, 2002). The majority of individuals with CRC (n = 33) were assessed before chemotherapy or radiation therapy.
Group Differences
Group differences in key cognitive variables and possible covariates are presented in Tables 2 and 3. On the ANT, the CRC group did not differ from controls on overall mean accuracy (p > 0.05) but had slower overall response times for correct answers compared to controls that approached significance (p = 0.06). Subsequent analyses of response times found that the mean response times for neutral flanker conditions were significantly (p < 0.05) slower in the individuals with CRC versus controls, suggesting that individuals in the CRC group had more difficulty discriminating the direction of the arrow when flanked by two straight lines on either side, a task that requires attention (Eriksen & Eriksen, 1974; Fan et al., 2002).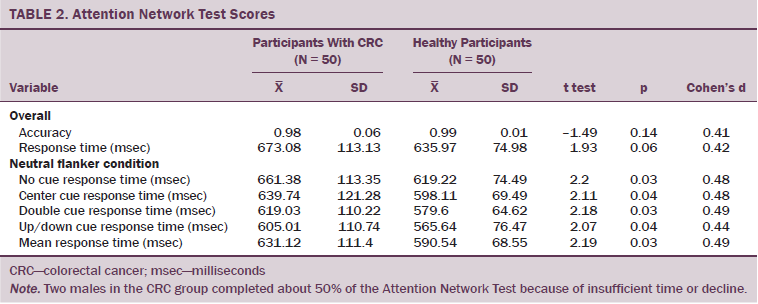
On DSF, TMA, and the attention composite score, individuals with CRC performed significantly worse compared to controls (p < 0.05). No significant differences were seen between the groups on DSB, TMB, or TMA minus TMB (p > 0.05). Finally, on the delayed measure of verbal memory, no significant differences were seen between groups on the RAVLT (p = 0.86). Together these findings suggest that individuals with CRC performed worse on measures of attention and cognitive control but not long-term memory.
[[{"type":"media","view_mode":"media_original","fid":"21901","attributes":{"alt":"","class":"media-image","height":"486","typeof":"foaf:Image","width":"760"}}]]
Those with CRC versus controls had significantly lower scores on the AFI self-report, indicating that individuals with CRC perceived lower effectiveness on everyday tasks requiring attention and cognitive control (p < 0.01). In contrast, on the self-report measure of memory, EMQ, no significant difference was seen between groups on perceived memory functioning (p = 0.47).
On the POMS-BF, results from comparative analyses indicated that individuals with CRC reported more anxiety and greater fatigue than healthy controls (p < 0.01). Finally, the CRC group reported higher depressed mood than the controls; however, the difference between the groups only approached significance (p = 0.06).
Predictors of Cognitive Impairment and Complaints
Multiple regression models were constructed to further assess the relationship between CRC diagnosis (independent variable) and cognitive measures (dependent variable), controlling for potential covariates. Cognitive measures included the attention composite score, the RAVLT delayed recall trial, the AFI, and the EMQ. Potential covariates included variables that were independently correlated (absolute r > 0.25, p < 0.05), with cognitive measures (age, education, anxiety, depressed mood, and fatigue) and one variable that differed between the groups (psychoactive medications) (see Table 4). Some of these variables (anxiety, depressed mood, and fatigue) were correlated and shared some variance but were sufficiently independent to include in the regression model. Gender also was included in the models because cognitive and behavioral differences have been observed between men and women (Lezak et al., 2012). In total, regression models included seven potential covariates. They were age, education, gender, anxiety, depressed mood, fatigue, and psychoactive medications. Regression models are presented in Tables 5 and 6.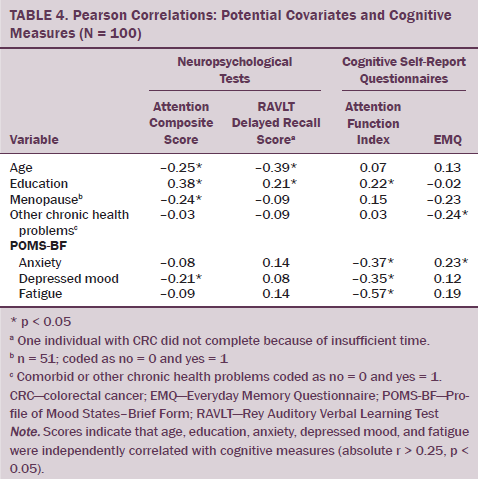
To assess the ability of CRC to predict attention and cognitive control performance after controlling for potential covariates, a regression analysis was performed using the attention composite score as the dependent variable and cancer diagnosis and potential covariates as independent variables. Independent variables accounted for 27% of the variance in the attention composite score (F[8, 91] = 4.29, p < 0.001). Of this variance, a significant portion was associated with CRC diagnosis, age, and education (p < 0.05). Findings indicated that having CRC, older age, and fewer years of education had a significant association with lower attention and cognitive control performance, controlling for potential covariates.
[[{"type":"media","view_mode":"media_original","fid":"21861","attributes":{"alt":"","class":"media-image","height":"468","typeof":"foaf:Image","width":"476"}}]]
For long-term memory performance, a similar regression model using the RAVLT delayed recall trial score as the dependent variable and cancer diagnosis and potential covariates as independent variables was performed. Independent variables accounted for 31% of the variance in the RAVLT delayed recall trial score (F[8, 90] = 5.1, p < 0.001). Of this variance, a significant portion was associated with age, education, and gender (p < 0.05) but not CRC diagnosis (p = 0.97). Findings indicate that older age, fewer years of education, and male gender had a significant association with lower long-term memory performance after controlling for potential covariates.
[[{"type":"media","view_mode":"media_original","fid":"21866","attributes":{"alt":"","class":"media-image","height":"417","typeof":"foaf:Image","width":"505"}}]]
For self-reported attention and cognitive control function, a similar regression model using the AFI score as the dependent variable and cancer diagnosis and potential covariates as independent variables was performed. The independent variables accounted for 38% of the variance in the self-report AFI (F[8, 91] = 6.91, p < 0.001). Of note, significant variance was only associated with fatigue and not CRC diagnosis or any other covariates included in the model. Findings indicate that increased fatigue had a significant association with lower perceived effectiveness on everyday activities requiring attention and cognitive control. For perceived memory function, a similar regression model using the self-report EMQ was performed and did not reach significance (F[8, 91] = 1.17, p = 0.33).
Discussion
Cognitive Deficits in Colorectal Cancer
The current study examined cognitive abilities of individuals with CRC to clarify prior suggestive evidence of dysfunction in this understudied population. The current study found that individuals with CRC had worse performance on tasks of attention and cognitive control, but not long-term memory, compared with healthy controls without a diagnosis of cancer. Similarly, individuals with CRC also reported less effectiveness with activities requiring attention and cognitive control but not self-reported memory abilities compared to healthy controls.
The finding that individuals with CRC performed worse on measures of attention and cognitive control provides new evidence of cognitive impairment in CRC and is consistent with prior reports in individuals with CRC receiving treatment for locally advanced and metastatic disease (Andreis et al., 2013; Cruzado et al., 2014; Walker et al., 1996). In particular, Walker et al. (1996) found that individuals with CRC receiving chemotherapy with or without immunotherapy (5-fluorouracil and leucovorin with or without interleukin-2) experienced slower reaction times to a visual stimulus and a reduced ability to sustain attention on the Cognitive Drug Research Computerized Assessment System. Cruzado et al. (2014) found that about a third of individuals with CRC were impaired on the TMT (31% TMA, 39% TMB) before, immediately after, and six months after adjuvant chemotherapy (FOLFOX4). Finally, Andreis et al. (2013) did not observe anticipated practice effects on the TMB test after individuals with CRC received adjuvant chemotherapy (FOLFOX4).
To the researchers’ knowledge, this is the first study to assess subjective cognitive complaints in individuals with CRC. The finding that individuals with CRC perceived their function on everyday tasks requiring attention and cognitive control to be worse than controls is consistent with research reports in other cancer populations (Cimprich, 1999; Ganz et al., 2013). In addition, the finding that participants with CRC performed and perceived their function to be worse than controls on measures of attention and cognitive control is consistent with emerging data and may reflect the use of a domain-specific self-report measure (Ganz et al., 2013).
The researchers anticipated that verbal long-term memory would be negatively affected based on previous findings in individuals with CRC (Cruzado et al., 2014), as well as findings from other cancer populations (Wefel et al., 2011), but this was not the case. A possibility is that because the RAVLT materials were learned at the beginning of the testing session, performance may have been optimal and less susceptible to fatigue than if the lists had been learned later in the session. However, the absence of impairment on the RAVLT is consistent with self-reported memory abilities, which also showed no indication of memory problems. Alternatively, the measures used to assess memory may not have been sufficiently sensitive to detect changes in function in this highly educated sample of men and women. Because of the inconsistent results pertaining to this measure, additional research on memory effects in individuals with CRC would be valuable.
Characteristics Associated With Cognitive Deficits
Regression analyses found that, after controlling for the influence of possible covariates, having CRC was a significant predictor of worse attention and cognitive control but not memory function. These findings are consistent with the comparative analyses and are important because they provide additional evidence that individuals with CRC are vulnerable to attention and cognitive control problems.
Age, education, and gender also were found to be significant predictors of cognitive function. Specifically, age and education were significant predictors of attention, cognitive control, and memory performance, and gender also was a significant predictor of memory performance. The finding that older age and fewer years of education were associated with poorer cognitive performance but not self-report is consistent with prior studies in individuals with cancer and healthy adults (Ahles et al., 2010; Cimprich, 1998; Cimprich, So, Ronis, & Trask, 2005; Lezak et al., 2012; Merriman et al., 2010). The finding that male gender was associated with poorer performance on the RAVLT but not the attention composite score or subjective measures of cognitive function is consistent with prior literature in healthy adults (Lezak et al., 2012).
Unexpectedly, fatigue, and not diagnosis of CRC, was a significant predictor of cognitive complaints on the attention and cognitive control self-report measure. One possible explanation for this finding is that participants reporting fatigue may have been affected by a common physiologic immune response to the cancer or other health problems and stressful events that can cause impairments in cognitive function regardless of source. Specifically, individuals with fatigue may be suffering from a cluster of cytokine-induced symptoms and behavioral changes (Cleeland et al., 2003). The finding that fatigue was not a significant predictor of objective performance on NP measures may suggest that objective measures are less sensitive to subtle deficits in attentional capacity and cognitive control perceived by the individual or that subtle changes in fatigue may not affect NP test performance. Continued research is needed to examine the relationship between fatigue and cognition in individuals with CRC.
In the current study, medications that could affect cognitive function and psychological distress were not associated with cognitive dysfunction or complaints. However, less than half of the study participants were taking psychoactive medications and the anxiety and depressed mood subscales were in the low to moderate range. Consequently, the low number of participants taking psychoactive medication and the low levels of distress may have been insufficient to affect attention and memory function. Nevertheless, these variables warrant further investigation in studies examining cognitive function in individuals with CRC. Specifically, the influence of psychoactive medication, as well as disease- or treatment-related symptom distress not included in the current study (e.g., pain, physical symptoms) on cognitive function needs to be further examined.
Limitations
The current study included theory-based NP tests and cognitive self-report measures, an adequate sample size, a healthy comparison group, and rigorous analytic methods to assess cognitive function in individuals with CRC and to identify possible factors associated with cognitive effects in CRC. The current study was limited by a cross-sectional design, the inclusion of individuals with varying stages of CRC, and the inclusion of a small number of individuals receiving adjuvant therapy. Importantly, although the study examined differences in attention and memory between individuals with and without cancer, it was not sufficiently powered to examine potential differences in cognition related to stage of disease or cancer treatments. In addition, although the study assessed multiple factors that could influence cognition, it did not assess all disease- or treatment-related factors (e.g., anemia) (Bender & Thelen, 2013).
Implications for Nursing
Despite its limitations, the current study provides important evidence that individuals with CRC are vulnerable to problems in attention and cognitive control. Because of the effects of these problems on an individual’s ability to function and cope with cancer, oncology nurses have a critical role in assessing for cognitive changes and intervening to optimize function. No empirically validated clinical cognitive assessments or interventions exist (Jansen, 2013; Von Ah, Jansen, Allen, Schiavone, & Wulff, 2011). The AFI, used in the current study, may hold promise as a clinical tool to assess cognitive complaints in CRC because it is brief, easy to use, and a sensitive instrument with established reliability and validity in cancer populations (Cimprich et al., 2011). For interventions, oncology nurses can validate the individual’s experience, identify and manage treatable factors associated with cognitive symptoms (e.g., fatigue), and provide education about cognitive changes in CRC (Jansen, 2013). Oncology nurses also can support individuals with CRC by sharing coping strategies that have been identified as beneficial by other cancer survivors (Von Ah, Storey, Jansen, & Allen, 2013). Such strategies include writing things down, avoiding multitasking, and seeking support from others (Von Ah et al., 2013). Finally, research is needed to validate findings, identify cognitive assessments for the clinical setting, and develop interventions to treat attention and cognitive control deficits in individuals with CRC.
References
Ahles, T.A., Saykin, A.J., McDonald, B.C., Li, Y., Furstenberg, C.T., Hanscom, B.S., . . . Kaufman, P.A. (2010). Longitudinal assessment of cognitive changes associated with adjuvant treatment for breast cancer: Impact of age and cognitive reserve. Journal of Clinical Oncology, 28, 4434–4440. doi:10.1200/JCO.2009.27.0827
American Cancer Society. (2014). Colorectal cancer facts and figures 2014–2016. Retrieved from http://www.cancer.org/acs/groups/content/documents/document/acspc-04228…
American Joint Committee on Cancer. (2002). AJCC cancer staging manual (6th ed.). Retrieved from https://cancerstaging.org/references-tools/deskreferences/Documents/AJC…
Andreis, F., Ferri, M., Mazzocchi, M., Meriggi, F., Rizzi, A., Rota, L., . . . Zaniboni, A. (2013). Lack of a chemobrain effect for adjuvant FOLFOX chemotherapy in colon cancer patients. A pilot study. Supportive Care in Cancer, 21, 583–590. doi:10.1007/s00520-012-1560-2
Bender, C.M., Sereika, S.M., Ryan, C.M., Brufsky, A.M., Puhalla, S., & Berga, S.L. (2013). Does lifetime exposure to hormones predict pretreatment cognitive function in women before adjuvant therapy for breast cancer? Menopause, 20, 922–929. doi:10.1097/GME.0b013e3182843eff
Bender, C.M., & Thelen, B.D. (2013). Cancer and cognitive changes: The complexity of the problem. Seminars in Oncology Nursing, 29, 232–237. doi:10.1016/j.soncn.2013.08.003
Cardinale, F., Chinellato, I., Caimmi, S., Peroni, D.G., Franceschini, F., Miraglia Del Giudice, M., & Bernardini, R. (2011). Perioperative period: Immunological modifications. International Journal of Immunopathology and Pharmacology, 24(Suppl. 3), S3–S12.
Cimprich, B. (1998). Age and extent of surgery affect attention in women treated for breast cancer. Research in Nursing and Health, 21, 229–238. doi:10.1002/(SICI)1098-240X(199806)21:3<229::AID-NUR6>3.0.CO;2-J
Cimprich, B. (1999). Pretreatment symptom distress in women newly diagnosed with breast cancer. Cancer Nursing, 22, 185–194. doi:10.1097/00002820-199906000-00001
Cimprich, B., & Ronis, D.L. (2001). Attention and symptom distress in women with and without breast cancer. Nursing Research, 50, 86–94. doi:10.1097/00006199-200103000-00004
Cimprich, B., So, H., Ronis, D.L., & Trask, C. (2005). Pre-treatment factors related to cognitive functioning in women newly diagnosed with breast cancer. Psycho-Oncology, 14, 70–78. doi:10.1002/pon.821
Cimprich, B., Visovatti, M., & Ronis, D.L. (2011). The Attentional Function Index—A self-report cognitive measure. Psycho-Oncology, 20, 194–202. doi:10.1002/pon.1729
Cleeland, C.S., Bennett, G.J., Dantzer, R., Dougherty, P.M., Dunn, A.J., Meyers, C.A., . . . Lee, B.N. (2003). Are the symptoms of cancer and cancer treatment due to a shared biologic mechanism? A cytokine-immunologic model of cancer symptoms. Cancer, 97, 2919–2925. doi:10.1002/cncr.11382
Cohen, J. (1992). Quantitative methods in psychology: A power primer. Psychological Bulletin, 112, 155–159. doi:10.1037/0033-2909.112.1.155
Cornish, I.M. (2000). Factor structure of the everyday memory questionnaire. British Journal of Psychology, 91, 427–438. doi:10.1348/000712600161916
Cruzado, J.A., López-Santiago, S., Martínez-Marín, V., José-Moreno, G., Custodio, A.B., & Feliu, J. (2014). Longitudinal study of cognitive dysfunctions induced by adjuvant chemotherapy in colon cancer patients. Supportive Care in Cancer, 22, 1815–1823. doi:10.1007/s00520-014-2147-x
Eriksen, B.A., & Eriksen, C.W. (1974). Effects of noise letters upon the identification of a target letter in a nonsearch task. Perceptions and Psychophysics, 16, 143–149. doi:10.3758/BF03203267
Fan, J., McCandliss, B.D., Sommer, T., Raz, A., & Posner, M.I. (2002). Testing the efficiency and independence of attentional networks. Journal of Cognitive Neuroscience, 14, 340–347. doi:10.1162/089892902317361886
Folstein, M.F., Folstein, S.E., & Fanjiang, G. (2000). Mini-Mental State Examination clinical guide. Lutz, FL: Psychological Assessment Resources.
Ganz, P.A., Kwan, L., Castellon, S.A., Oppenheim, A., Bower, J.E., Silverman, D.H.S., . . . Belin, T.R. (2013). Cognitive complaints after breast cancer treatments: Examining the relationship with neuropsychological test performance. Journal of the National Cancer Institute, 105, 791–801. doi:10.1093/jnci/djt073
Gazzaniga, M.S., Ivry, R.B., & Mangun, G.R. (2014). Cognitive neuroscience: The biology of the mind (4th ed.). New York, NY: W.W. Norton and Company.
Giovagnoli, A.R., Del Pesce, M., Masheroni, S., Simoncelli, M., Laiacona, M., & Capitani, E. (1996). Trail making test: Normative values from 287 normal adult controls. Italian Journal of Neurological Sciences, 17, 305–309. doi:10.1007/BF01997792
Han, R., Yang, Y.M., Dietrich, J., Luebke, A., Mayer-Pröschel, M., & Noble, M. (2008). Systemic 5-fluorouracil treatment causes a syndrome of delayed myelin destruction in the central nervous system. Journal of Biology. Retrieved from http://www.jbiol.com/content/7/4/12
James, W. (1890). The principles of psychology. New York, NY: H. Holt and Company.
Jansen, C.E. (2013). Cognitive changes associated with cancer and cancer therapy: Patient assessment and education. Seminars in Oncology Nursing, 29, 270–279. doi:10.1016/j.soncn.2013.08.007
Jansen, C.E., Dodd, M.J., Miaskowski, C.A., Dowling, G.A., & Kramer, J. (2008). Preliminary results of a longitudinal study of changes in cognitive function in breast cancer patients undergoing chemotherapy with doxorubicin and cyclophosphamide. Psycho-Oncology, 17, 1189–1195. doi:10.1002/pon.1342
Jung, M.S., & Cimprich, B. (2014). Cognitive deficits in Korean women treated with chemotherapy for breast cancer. Cancer Nursing, 37, E31–E42. doi:10.1097/NCC.0b013e3182980383
Kaplan, S., & Kaplan, R. (1989). Cognition and environment. Ann Arbor, MI: Ulrich.
Klampfer, L. (2011). Cytokines, inflammation and colon cancer. Current Cancer Drug Targets, 11, 451–464. doi:10.2174/156800911795538066
Koppelmans, V., Breteler, M.M., Boogerd, W., Seynaeve, C., Gundy, C., & Schagen, S.B. (2012). Neuropsychological performance in survivors of breast cancer more than 20 years after adjuvant chemotherapy. Journal of Clinical Oncology, 30, 1080–1086. doi:10.1200/JCO.2011.37.0189
Lehto, R.H., & Cimprich, B. (1999). Anxiety and directed attention in women awaiting breast cancer surgery. Oncology Nursing Forum, 26, 767–772.
Lezak, M.D., Howieson, D.B., Bigler, E.D., & Tranel, D. (2012). Neuropsychological assessment (5th ed.). New York, NY: Oxford University Press.
Mackie, M.A., Van Dam, N.T., & Fan, J. (2013). Cognitive control and attentional functions. Brain and Cognition, 82, 301–312.
MacLeod, J.W., Lawrence, M.A., McConnell, M.M., Eskes, G.A., Klein, R.M., & Shore, D.I. (2010). Appraising the ANT: Psychometric and theoretical considerations of the Attention Network Test. Neuropsychology, 24, 637–651. doi:10.1037/a0019803
McNair, D.M., Lorr, M., & Droppleman, L.F. (1992). Profile of Mood States. San Diego, CA: Educational and Industrial Testing Service.
Merriman, J.D., Jansen, C., Koetters, T., West, C., Dodd, M., Lee, K., . . . Miaskowski, C. (2010). Predictors of the trajectories of self-reported attentional fatigue in women with breast cancer undergoing radiation therapy. Oncology Nursing Forum, 37, 423–432. doi:10.1188/10.ONF.423-432
Merriman, J.D., Von Ah, D., Miaskowski, C., & Aouizerat, B.E. (2013). Proposed mechanisms for cancer- and treatment-related cognitive changes. Seminars in Oncology Nursing, 29, 260–269. doi:10.1016/j.soncn.2013.08.006
Miller, E.K. (2000). The prefrontal cortex and cognitive control. Nature Reviews Neuroscience, 1, 59–65. doi:10.1038/35036228
Petersen, S.E., & Posner, M.I. (2012). The attention system of the human brain: 20 years after. Annual Review of Neuroscience, 35, 73–89. doi:10.1146/annurev-neuro-062111-150525
Posner, M.I., & Snyder, C.R.R. (1975). Attention and cognitive control. In R.L. Solso (Ed.), Information processing and cognition: The Loyola symposium (pp. 55–85). New York, NY: Lawrence Erlbaum Associates.
Reitan, R.M. (1979). Trail Making Test manual for administration and scoring. Tucson, AZ: Reitan Neuropsychology Laboratory.
Royle, J., & Lincoln, N.B. (2008). The Everyday Memory Questionnaire-revised: Development of a 13-item scale. Disability and Rehabilitation, 30, 114–121. doi:10.1080/09638280701223876
Schaue, D., Micewicz, E.D., Ratikan, J.A., Xie, M.W., Cheng, G., & McBride, W.H. (2015). Radiation and inflammation. Seminars in Radiation Oncology, 25, 4–10. doi:10.1016/j.semradonc.2014.07.007
Small, B.J., Rawson, K.S., Walsh, E., Jim, H.S., Hughes, T.F., Iser, L., . . . Jacobsen, P.B. (2011). Catechol-O-methyltransferase genotype modulates cancer treatment-related cognitive deficits in breast cancer survivors. Cancer, 117, 1369–1376. doi:10.1002/cncr.25685
Squire, L.R. (2004). Memory systems of the brain: A brief history and current perspective. Neurobiology of Learning and Memory, 82, 171–177. doi:10.1016/j.nlm.2004.06.005
Tonini, G., Santini, D., Vincenzi, B., Borzomati, D., Dicuonzo, G., La Cesa, A., . . . Coppola, R. (2002). Oxaliplatin may induce cytokine-release syndrome in colorectal cancer patients. Journal of Biological Regulators and Homeostatic Agents, 16, 105–109.
Von Ah, D., Carpenter, J.S., Saykin, A., Monahan, P., Wu, J., Yu, M., . . . Unverzagt, F. (2012). Advanced cognitive training for breast cancer survivors: A randomized controlled trial. Breast Cancer Research Treatment, 135, 799–809. doi:10.1007/s10549-012-2210-6
Von Ah, D., Jansen, C., Allen, D.H., Schiavone, R.M., & Wulff, J. (2011). Putting Evidence Into Practice: Evidence-based interventions for cancer and cancer treatment-related cognitive impairment. Clinical Journal of Oncology Nursing, 15, 607–615. doi:10.1188/11.CJON.607-615
Von Ah, D., Storey, S., Jansen, C.E., & Allen, D.H. (2013). Coping strategies and interventions for cognitive changes in patients with cancer. Seminars in Oncology Nursing, 29, 288–299. doi:10.1016/j.soncn.2013.08.009
Walker, L.G., Wesnes, K.P., Heys, S.D., Walker, M.B., Lolley, J., & Eremin, O. (1996). The cognitive effects of recombinant interleukin-2 (rIL-2) therapy: A controlled clinical trial using computerised assessments. European Journal of Cancer, 32, 2275–2283.
Wang, K., Fan, J., Dong, Y., Wang, C.Q., Lee, T.M., & Posner, M.I. (2005). Selective impairment of attentional networks of orienting and executive control in schizophrenia. Schizophrenia Research, 78, 235–241. doi:10.1016/j.schres.2005.01.019
Wefel, J.S., Vardy, J., Ahles, T., & Schagen, S.B. (2011). International Cognition and Cancer Task Force recommendations to harmonise studies of cognitive function in patients with cancer. Lancet Oncology, 12, 703–708. doi:10.1016/S1470-2045(10)70294-1
About the Author(s)
Visovatti is a research fellow in the School of Nursing, Reuter-Lorenz is department chair and professor of psychology, Chang is the Hugh Cabot professor of surgery, and Northouse and Cimprich are both professor emerita in the School of Nursing, all at the University of Michigan in Ann Arbor. No financial relationships to disclose. All authors contributed to the conceptualization and design and manuscript preparation. Visovatti, Cimprich, Chang, and Northouse completed the data collection. Visovatti, Cimprich, and Reuter-Lorenz provided statistical support and analysis. Mention of specific products and opinions related to those products do not indicate or imply endorsement by the Oncology Nursing Forum or the Oncology Nursing Society. Visovatti can be reached at mvisovat@umich.edu, with copy to editor at ONFEditor@ons.org. Submitted April 2015. Accepted for publication July 24, 2015.